Ulnar Claw and Hand of Benediction are characteristic signs of nerve
injury. Although they look largely the same, the underlying pathology is
very different. In this article, we shall look at the basic anatomy,
and apply this to both cases, and thereby understanding the clinical
presentation of the two signs.
Ulnar Claw
This is a deformity that is mostly seen in long-term cases of a
lesion of the ulnar nerve. To explain it, we need to consider which
muscles are paralysed by a lesion at the wrist:
- Medial Two Lumbricals: Flexes the MCP (metacarpophalangeal joints) of the little and ring fingers. Extends the IP (interphalangeal joints) of the little and ring fingers
- Interossei: Abduct and adduct the fingers
- Hypothenar Muscles: Flex, adduct, and oppose the little finger
- Adductor Pollicis: Adducts the thumb
The key set of muscles that are paralysed are the lumbricals. There
is now a loss of flexion at the MCP joint and a loss of extension at the
IP joints.
This results in the ulnar claw; the MCP joints are hyperextended by
unopposed extension from the extensor digitorum, and the IP joints are
flexed by unopposed flexion from the flexor digitorum profundus. This
only occurs in the little and ring fingers as the lateral two lumbricals
are innervated by the median nerve.
Ulnar Paradox
Now consider at lesion of the ulnar nerve at the elbow. In addition to the muscles of the hand, these muscles are paralysed:
- Medial half of Flexor Digitorum Profundus: Flexes the IP joints of the ring and little fingers
- Flexor Carpi Ulnaris: Flexes and adducts the wrist
The ulnar claw will develop as before, but with one key difference.
The flexor digitorum profundus is paralysed, and there will not be any
flexion of the ring and little fingers. Now the ulnar claw only consists
of hyperextension at the MCP joints, giving a less evident claw hand.
This is known as the ‘ulnar paradox’ – you would expect a
more debilitating injury to produce a more pronounced deformity, but in
fact the opposite occurs.
Hand of Benediction
Hand of benediction occurs as a result of injury to the median nerve.
It is only apparent if the patient is asked to make a fist.
Result of median nerve damage
Again, we need to consider the muscles paralysed if a lesion to the median nerve occurs at the wrist:
- All the flexors in the anterior compartment of the arm, except the medial half of the flexor digitorum profundus and the flexor carpi ulnaris.
- Lateral Two Lumbricals: Flexes the MCP (metacarpophalangeal joints) of the middle and index fingers. Extends the IP (interphalangeal joints) of the middle and index fingers.
If the patient is asked to make a fist, they will be able to flex the
little and ring fingers. This action is performed by the medial half of
the flexor digitorum profundus and the medial two lumbricals.
The patient will not be able to flex the index and middle fingers.
Thus, the patient displays a claw shape, where the little and ring
fingers and flexed, the index and middle fingers extended.
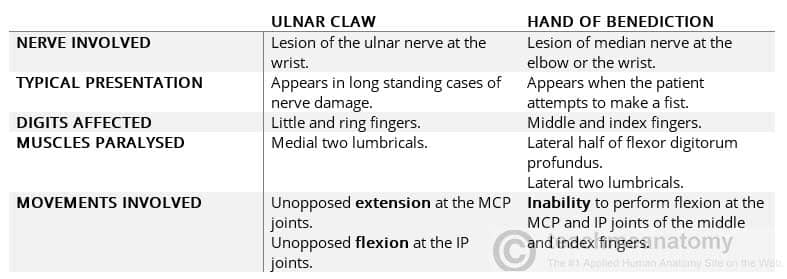
Contrasting Ulnar Claw and Hand of Benediction
At a first glance, distinguishing between the two can be difficult,
but there are numerous differences between ulnar claw and hand of
benediction.